
Enhancing organ donation in SA – beyond public awareness
Dr. Harriet Etheredge
Posted on May 22, 2017
My post from last week generated some debate. Opinions regarding whether or not “Bypass movie” could damage SA’s transplant system are polarised. It’s an interesting discussion, but no response has been convincing enough to change my mind – I still think that the film and its advertising have propensity to harm. I’m not going into any more detail; rather, I want to focus on other aspects of transplant which I think are sometimes overlooked.
Why is public awareness in SA such a challenge?
SA is unique and complex. 11 languages are spoken; literacy levels, socio-political and socio-economic statuses differ vastly and people hold differing socio-cultural and religious beliefs. This diversity makes comprehensive public awareness a huge challenge. Moreover, whilst public awareness is important, it is not the panacea for increasing transplant numbers in SA (imho – this really should be the ultimate goal). Other challenges at ‘clinic level’ also need to be addressed. Some colleagues and I discussed these in a recent academic article.
What’s happening at ‘clinic level’ in our hospitals?
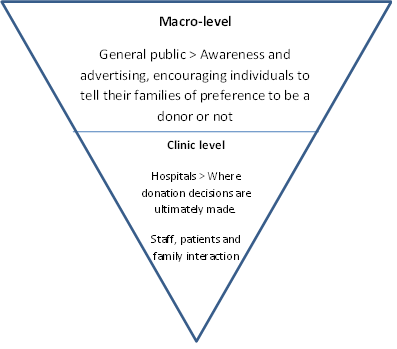
We can conceptualise ‘clinic level’ by thinking of transplant in many layers, like the figure below. Public awareness is an umbrella, but it really comes down to the hospital setting. Here, patients and their families interact with health professionals and consent is sought.
A layered transplant system
In my PhD research[1] I identified a number of ‘barriers to transplant’ at clinic level. A ‘barrier to transplant’ is a situation or perception that might prevent health staff from referring potential donors or might prevent families from consenting to organ donation. Barriers are not always related to public awareness. Rather, they are functions of the hospital environment and the ways information is provided in that setting. You can see these in the figure below.
Clinic level barriers to transplant

What should be done?
In order to overcome some of these barriers here’s what I think we need:
- For all health professionals – Robust training on having difficult conversations with (and breaking bad news to) patients and families
- Focus on empowering and educating nurses – as those spending the most time with patients, nurses are in a unique position to facilitate transplant but they need a solid framework in which to do this.
- A “mandatory referral system” where all patients who are diagnosed as brain-stem dead – or in whom brain-stem death is imminent – are referred to a transplant coordinator. A transplant coordinator is usually a specialist nurse who has trained in transplant and has the skills to ask consent from families.
- A more extensive transplant curriculum for medical and nursing students
- Governmental commitment to clarify transplant legislation, legislate mandatory referral and increase the number of transplant coordinators – especially at state hospitals.
For much more detailed information about the barriers to transplant and recommendations in the blog, please see this article or contact me on the Contact page.
The views published in this blog are entirely my own (informed) opinions. They are open to debate, discussion and disagreement.
[1] A PhD is a HUGE research project where the candidate goes about exploring or examining a topic in a manner that must be novel and original, and which must significantly add to the body of evidence on a particular topic. In SA, a PhD thesis is generally examined by a number of experts in the field – in my case, a very widely cited transplant professional from Australia, another from SA and a third examiner from Wits. A PhD is also supervised by experts, in my case two professors, one of whom is amongst only a handful of NRF A-rated social scientists in SA. You can see my thesis – all 500 pages of it – here. Happy reading!
